You’ve been prescribed a tube of cream for your eczema or psoriasis, but you’re hesitating. You’ve heard the rumors about topical steroids causing permanent damage, specifically that they make your skin paper-thin and fragile. It’s a valid fear. Nobody wants to trade one skin problem for another. But here is the reality: these medications are among the most effective tools dermatologists have, and when used correctly, they are incredibly safe.
The problem isn’t the medicine itself; it’s how we use it. Most side effects, including skin atrophy (thinning), come from using the wrong strength, applying too much, or leaving it on sensitive areas like the face for too long. Let’s clear up the confusion so you can treat your condition without anxiety.
Understanding Potency: Not All Creams Are Created Equal
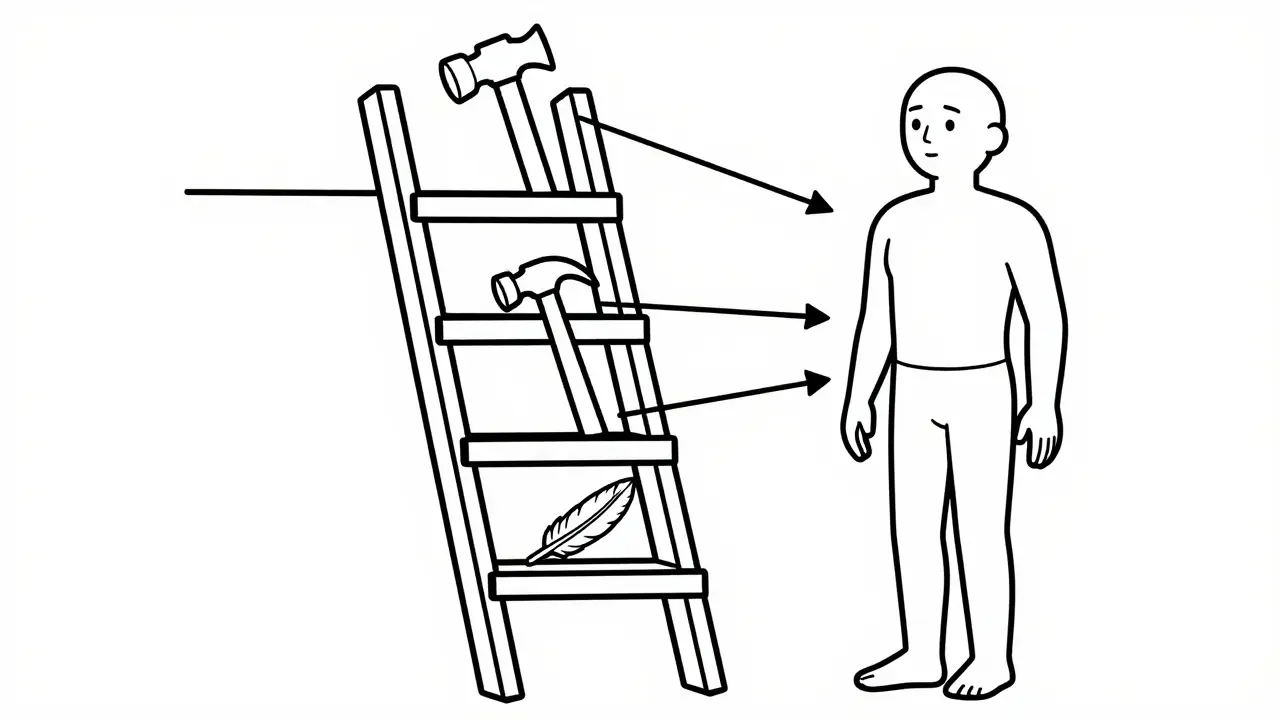
Think of topical corticosteroids like a ladder. They range from Class VII (mild) to Class I (super-potent). Using a Class I steroid on your eyelid is like using a sledgehammer to crack a nut-it causes unnecessary damage. Conversely, using a mild steroid on thick, plaque-like psoriasis on your elbows might do nothing at all.
| Potency Class | Strength Level | Typical Examples | Best For |
|---|---|---|---|
| Class I - II | Super-Potent / Very Potent | Clobetasol, Betamethasone dipropionate | Thick plaques on palms, soles, or elbows |
| Class III - IV | Moderately Potent | Triamcinolone, Mometasone | Trunk, arms, legs (general body) |
| Class V - VI | Low Potency | Hydrocortisone 1%, Desonide | Face, groin, underarms, children |
| Class VII | Mild | Hydrocortisone 0.5% | Eyelids, delicate facial skin, minor rashes |
The key takeaway? Match the potency to the thickness of the skin. The skin on your palms and soles is millimeters thick and can handle stronger meds. The skin on your face and groin is thin and absorbs medication rapidly, making it prone to side effects if you use anything stronger than low-potency formulas.
The Fingertip Unit: Stop Guessing, Start Measuring
One of the biggest reasons people experience side effects is simple over-application. We tend to squeeze out a glob because we want the rash to go away fast. But more is not better. In fact, studies show that applying more than the recommended amount doesn't speed up healing; it just increases the risk of absorption into your bloodstream and local skin damage.
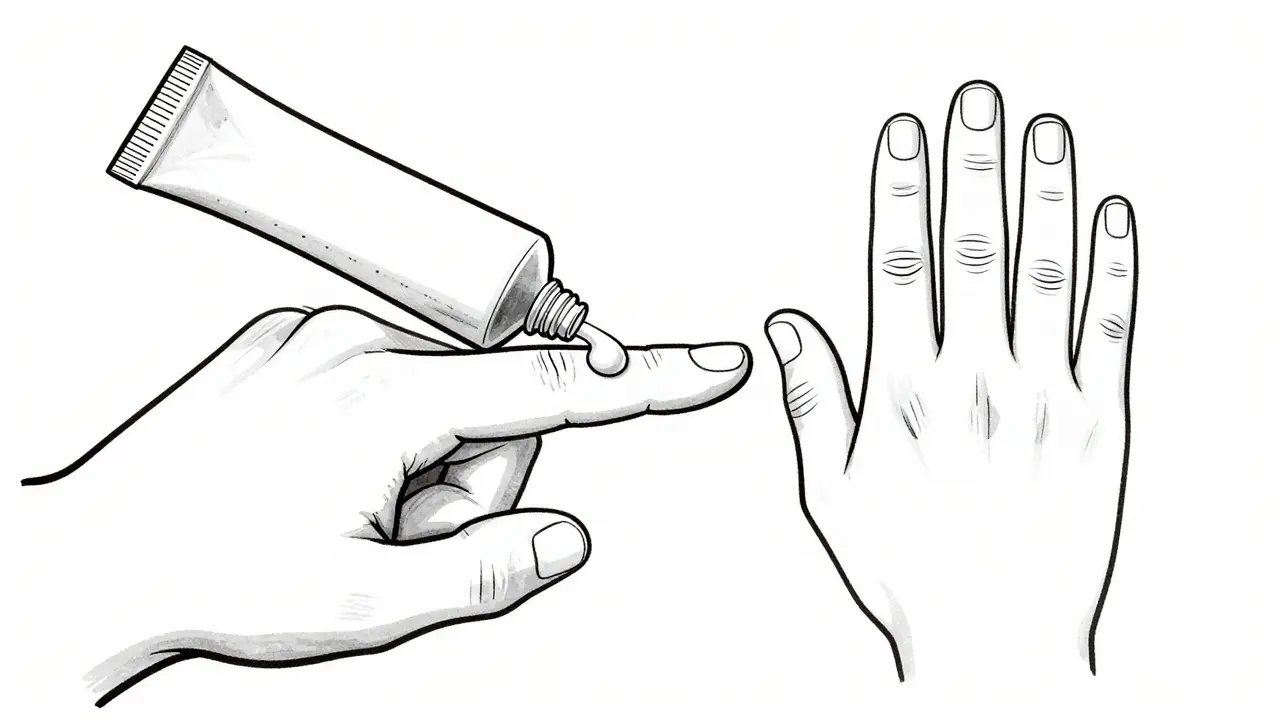
To measure correctly, use the Fingertip Unit (FTU), which is a standardized measurement defined as the amount of ointment squeezed from the tip of an adult's index finger to the first crease. One FTU covers an area roughly the size of two adult hands pressed together (about 30 square centimeters).
- One hand (front and back): 1 FTU
- One arm: 3 FTUs
- One leg: 6 FTUs
- Entire trunk (chest and back): 7-14 FTUs
If you’re treating a small patch of eczema on your knee, you likely only need half an FTU. A thin layer that disappears when rubbed in is enough. If you can still see white residue, you’ve used too much.
Skin Thinning: What Actually Happens?
Let’s address the elephant in the room: atrophy. When you use potent steroids for too long, especially on thin skin, the medication suppresses the production of collagen and elastin. This leads to:
- Visible blood vessels: The skin becomes translucent, revealing capillaries underneath (telangiectasia).
- Stretch marks: Known as striae, these look like purple or red lines that fade to silver.
- Easy bruising: The skin loses its structural integrity.
- Wrinkling: Premature aging of the treated area.
Here is the good news: this is largely preventable. According to guidelines from the American Academy of Family Physicians, high-potency steroids should rarely be used for more than two weeks continuously. For milder steroids, the window is longer, but continuous daily use for months without a break is where problems start.
The Step-Down Strategy: Smart Long-Term Management
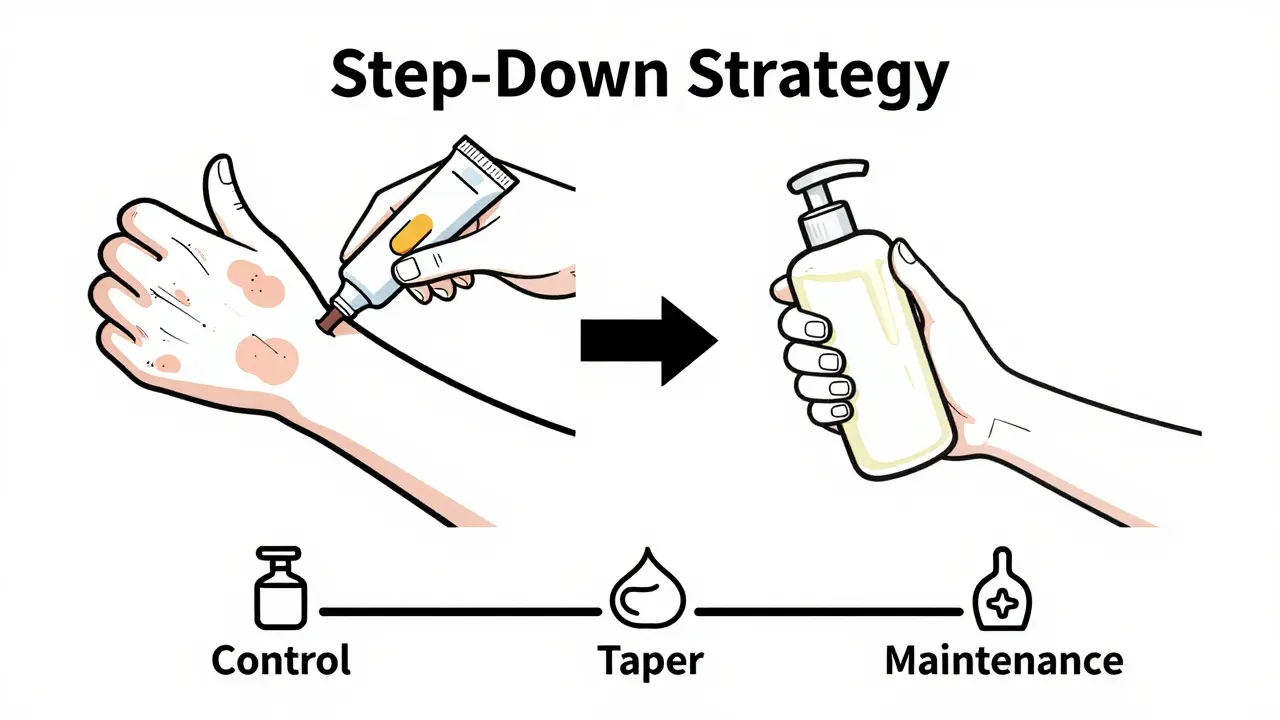
If you have a chronic condition like atopic dermatitis, you can’t just stop using steroids forever once the flare-up clears, or it will often return. The solution isn’t avoidance; it’s strategy. Dermatologists recommend a "step-down" approach.
- Control Phase: Use a moderate-to-strong steroid for 1-2 weeks to knock out the inflammation completely.
- Taper Phase: Switch to a lower-potency steroid (e.g., from triamcinolone to hydrocortisone) for another week.
- Maintenance Phase: Stop the steroid entirely and rely on emollients (moisturizers) or non-steroidal alternatives like calcineurin inhibitors (tacrolimus/pimecrolimus) for sensitive areas.
This method keeps the skin calm while minimizing the time any single area is exposed to strong anti-inflammatory agents.
Vehicle Matters: Cream vs. Ointment
The base of your medication changes how it works. An ointment is an oil-based preparation that creates an occlusive barrier, trapping moisture and increasing drug absorption. Because it seals the skin, ointments are more potent per gram than creams. They are excellent for dry, scaly patches on elbows or knees but terrible for the face or hairy scalp because they feel greasy and can clog pores, leading to acne.
Creams are water-based mixtures that absorb quickly and are less occlusive. They are better for moist or weeping lesions and are generally preferred for the face and body because they feel lighter. If you have very dry skin, apply your moisturizer first, wait 20 minutes, then apply the steroid. Applying them simultaneously dilutes the medication and reduces its effectiveness.
Sensitive Zones: Where to Be Extra Careful
Your face, groin, and armpits are different beasts. The skin here is thinner and has a higher surface-area-to-volume ratio for absorption. Here is what you need to know:
- Face: Only use mild steroids (Class VI-VII) for short periods (max 5-7 days). Stronger steroids here can cause perioral dermatitis (a red, bumpy rash around the mouth) or even glaucoma/cataracts if near the eyes.
- Eyelids: Extremely risky. Even mild steroids can thin the skin significantly here. Consult a doctor before applying anything to the eyelid margin.
- Groin/Armpits: These areas are warm and moist, which enhances absorption. Use low-potency steroids sparingly and consider non-steroidal options like tacrolimus if the issue persists.
When to See a Doctor
You should seek professional advice if:
- You’ve been using the same steroid for more than two weeks with no improvement.
- You notice visible veins, stretch marks, or significant thinning in the treated area.
- The rash spreads despite treatment.
- You are pregnant or breastfeeding, as systemic absorption can occur with large surface area applications.
Remember, topical steroids are powerful allies, not enemies. By respecting their potency, measuring your dose, and knowing when to step down, you can manage your skin condition effectively without compromising its health.
How long does it take for skin thinning to reverse after stopping topical steroids?
Mild thinning often improves within a few weeks to months after discontinuing the medication. However, severe atrophy with visible blood vessels or deep stretch marks may be permanent. This is why prevention through proper usage is critical.
Can I use topical steroids on my face for eczema?
Yes, but only with low-potency steroids (like hydrocortisone 1% or desonide) and for short durations (no more than 5-7 days). Avoid strong steroids on the face to prevent perioral dermatitis and skin atrophy.
What is the difference between a cream and an ointment for steroids?
Ointments are oil-based and more occlusive, making them more potent and better for dry, thick skin. Creams are water-based, absorb faster, and are less greasy, making them suitable for the face, body, and moist areas.
Is it safe to use topical steroids on children?
Yes, but caution is required. Children have a higher surface-area-to-body-weight ratio, increasing absorption risk. Always use the lowest potency effective for the condition and strictly follow duration limits set by a pediatrician.
What are non-steroidal alternatives for sensitive areas?
Calcineurin inhibitors like tacrolimus (Protopic) and pimecrolimus (Elidel) are common non-steroidal options. They reduce inflammation without causing skin thinning, making them ideal for the face, eyelids, and groin.
