Imagine your heart’s fuel lines slowly clogging up like old pipes in an old house. That is essentially what happens with Coronary Artery Disease, commonly known as CAD. It is the number one killer worldwide, accounting for roughly 13% of all global deaths between 2000 and 2021 according to World Health Organization data. But here is the scary part: you can have severe blockages without feeling a thing until it is too late. The good news? We know exactly why it happens, how to spot the risks, and-most importantly-how to stop it or reverse its damage.
This isn't just about eating less butter. It is about understanding the biology of plaque, recognizing that 'stable' doesn't always mean 'safe,' and knowing which treatments actually work for your specific risk profile. Let's break down the mechanics of this silent threat so you can take control of your heart health.
The Root Cause: How Atherosclerosis Builds Up
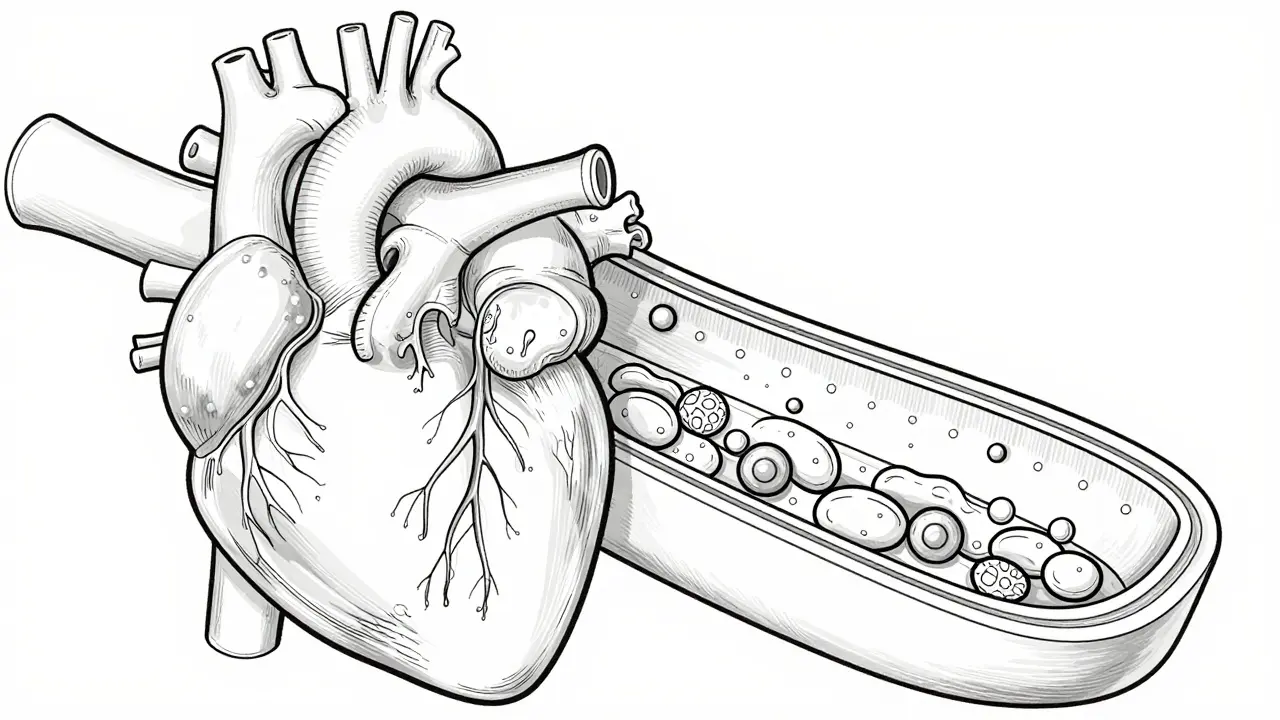
To understand CAD, you first need to understand Atherosclerosis. This is the process where fatty deposits, called atheromas, build up inside your arteries. Think of your arteries as flexible garden hoses. Over time, if there is high pressure, inflammation, or sticky debris (like cholesterol), the inner lining gets damaged. Your body tries to repair this damage by sending immune cells and smooth muscle cells to the site. These cells, along with fats and calcium, form a hard, crusty plaque.
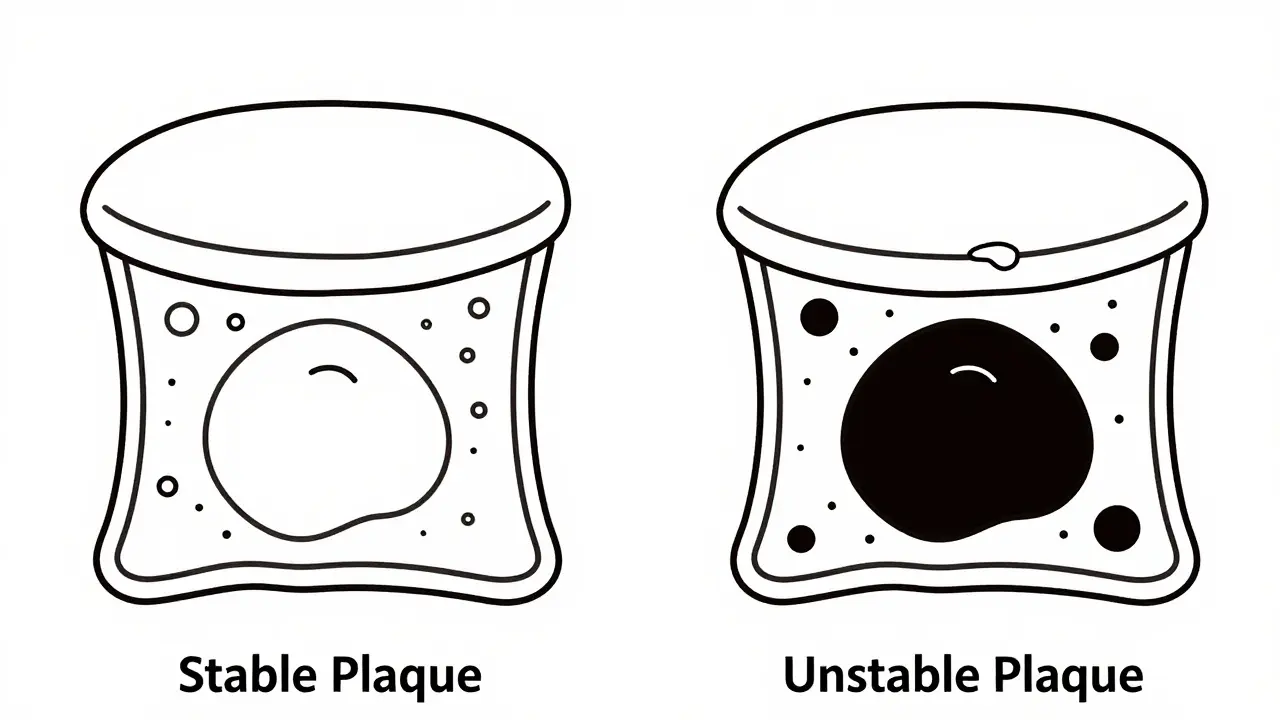
Here is where it gets tricky. Not all plaques are created equal. Doctors look at two main types:
- Stable Plaques: These have a thick fibrous cap and fewer lipids. They usually narrow the artery lumen by more than 50%. Because they are stable, they cause predictable symptoms, like chest pain when you exercise, because the blood flow is physically restricted.
- Unstable (Vulnerable) Plaques: These are the real danger. They have a thin fibrous cap, a large lipid core, and lots of inflammatory macrophages. Surprisingly, these often narrow the vessel by less than 50%. You might not feel any pain because blood can still squeeze through. But if that thin cap ruptures, it triggers a blood clot that can completely block the artery instantly, causing a heart attack.
This distinction is crucial. A person with a 90% blockage might be safer from sudden death than someone with a 40% blockage made of unstable, rupture-prone plaque. This is why doctors don't just look at stenosis percentage; they look at plaque stability.
Risk Factors: Who Is in the Danger Zone?
You cannot change your age or genetics, but you can control many of the drivers behind atherosclerosis. The 2023 ACC/AHA guidelines highlight several key risk factors that significantly increase your chances of developing Chronic Coronary Disease (CCD).
| Risk Factor | Why It Matters | Actionable Step |
|---|---|---|
| High LDL Cholesterol | LDL particles penetrate the arterial wall, triggering inflammation and plaque formation. | Aim for LDL below 70 mg/dL if you have existing heart disease. |
| Hypertension (High Blood Pressure) | Damages the endothelial lining of arteries, making them susceptible to plaque buildup. | Keep BP under 130/80 mmHg through diet, exercise, and medication if needed. |
| Diabetes | High blood sugar damages blood vessels and nerves, accelerating atherosclerosis. | Maintain HbA1c levels within target range (usually <7%). |
| Smoking | Chemicals in smoke cause immediate endothelial dysfunction and increase clotting risk. | Quit smoking entirely; benefits begin within weeks. |
| Elevated BMI / Obesity | Associated with inflammation, higher blood pressure, and worse lipid profiles. | Lose even 5-10% of body weight to reduce cardiac strain. |
| Chronic Kidney Disease | Reduced kidney function (eGFR <60 ml/min) is a major independent risk factor. | Monitor kidney function regularly; manage blood pressure tightly. |
It is also important to note that conditions like atrial fibrillation and heart failure with preserved ejection fraction (HFpEF) place patients in a higher risk category. In fact, research shows that 60% of patients exhibit high-risk features, and 75% of primary cardiovascular events occur in this group. If you have multiple vascular beds involved (for example, carotid and coronary arteries), your risk skyrockets.
Diagnosis: Seeing What You Cannot Feel
Because CAD can be silent, diagnosis often relies on provoking the heart into showing its limits or visualizing the arteries directly. Here are the standard tools doctors use:
- Electrocardiogram (ECG): A quick test that records the electrical activity of your heart. It can show signs of past heart attacks or current ischemia (lack of oxygen).
- Stress Tests: You walk on a treadmill or ride a stationary bike while your heart rate and ECG are monitored. If your heart demands more oxygen than the narrowed arteries can supply, changes appear on the monitor or you experience symptoms.
- Coronary Angiography: This is the gold standard for visualization. A catheter is threaded into your coronary arteries, and contrast dye is injected. X-rays then show exactly where the blockages are and how severe they are.
- Ankle-Brachial Index (ABI): While primarily used for Peripheral Artery Disease (PAD), PAD and CAD often coexist. An abnormal ABI suggests widespread atherosclerosis, increasing the likelihood of CAD.
Newer guidelines also emphasize looking for Ischemia with Nonobstructive Coronary Arteries (INOCA). This affects many patients, particularly women, who have typical chest pain but normal-looking arteries on angiography. It suggests microvascular dysfunction rather than large-vessel blockage, requiring different management strategies.

Treatments: From Lifestyle to Surgery
Treating CAD is not a one-size-fits-all approach. It depends on your risk stratification: Low (<1% yearly risk), Intermediate (1-3%), or High (>3%). The goal is to prevent plaque rupture, stabilize existing plaque, and restore blood flow if necessary.
1. Lifestyle Modifications (The Foundation)
No medication works well if lifestyle factors are ignored. This means adopting a heart-healthy diet (rich in vegetables, fruits, whole grains, and lean proteins), engaging in regular aerobic exercise (at least 150 minutes per week), and managing stress. Quitting smoking is the single most effective step you can take if you are a smoker.
2. Medications (The Shield)
For most patients, lifelong medication is required. Common classes include:
- Statins: Lower LDL cholesterol and, crucially, stabilize plaque by reducing inflammation within the arterial wall.
- Antiplatelets (e.g., Aspirin): Prevent blood clots from forming on ruptured plaques.
- Beta-blockers and ACE Inhibitors: Reduce the heart's workload and lower blood pressure.
- Anticoagulants: Used if you also have atrial fibrillation to prevent stroke and systemic clots.
The 2023 guidelines emphasize personalized antithrombotic therapy. For high-risk patients, dual antiplatelet therapy might be recommended for a longer duration, balanced against bleeding risks.
3. Procedures (The Fix)
If lifestyle and meds aren't enough, or if you have critical blockages, procedures come into play:
- Percutaneous Coronary Intervention (PCI): Also known as angioplasty and stenting. A balloon opens the blocked artery, and a mesh tube (stent) is placed to keep it open. Drug-eluting stents release medication to prevent scar tissue growth.
- Coronary Artery Bypass Grafting (CABG): Open-heart surgery where surgeons take a healthy vessel from another part of your body (like the leg or chest) and graft it to bypass the blocked section. This is often preferred for multi-vessel disease or diabetes patients.
The Future: Cardio-Oncology and Personalized Care
As people live longer, we are seeing more complex cases. The field of cardio-oncology is emerging because cancer survivors often develop heart issues due to chemotherapy or radiation. Conversely, heart patients may develop cancer. Managing both requires specialized care that balances life-saving cancer treatments with heart protection.
Furthermore, the focus is shifting toward precision medicine. Instead of just treating "high cholesterol," doctors are looking at genetic markers, plaque composition via advanced imaging, and individual risk scores to tailor therapies. The message is clear: CAD is manageable, but it requires vigilance, adherence to treatment, and a proactive partnership with your healthcare provider.
Can coronary artery disease be reversed?
While you cannot completely remove calcified plaque, aggressive lifestyle changes and medications like statins can stabilize plaque and sometimes shrink the lipid core, reducing the risk of rupture. Revascularization procedures like PCI or CABG restore blood flow but do not cure the underlying atherosclerosis.
What is the difference between stable and unstable angina?
Stable angina occurs predictably during exertion and resolves with rest, indicating fixed blockages. Unstable angina occurs at rest, is unpredictable, and signals a high risk of imminent heart attack due to plaque rupture or severe narrowing.
Do I need a stent if my blockage is only 40%?
Usually, no. Blockages under 50% rarely benefit from stenting unless they are causing significant ischemia proven by functional testing. Treatment focuses on medication and lifestyle to prevent progression. However, if the plaque is unstable, medical management becomes even more critical.
How does diabetes affect coronary artery disease?
Diabetes accelerates atherosclerosis by damaging blood vessel linings and promoting inflammation. Diabetics often have diffuse disease affecting multiple arteries, making them higher candidates for bypass surgery (CABG) over stenting, and requiring stricter glucose and lipid control.
What is INOCA and who gets it?
Ischemia with Nonobstructive Coronary Arteries (INOCA) refers to chest pain and reduced blood flow despite having no major blockages in the large coronary arteries. It is more common in women and involves dysfunction of the tiny microvessels supplying the heart muscle.
